
Case-Report | DOI: https://doi.org/10.31579/2578-8868/112
Neurosurgeon in Mexico City, Mexico
*Corresponding Author: Carlos Francisco Gutierrez Partida, Neurosurgeon in Mexico City, Mexico
Citation: Gutierrez Partida CF., Ramirez Leon. JF., Ramirez Martinez. CC (2020) Spinal Descompression Trhough a Tubular System with Assisted Endoscopy. J. Neuroscience and Neurological Surgery. 6(1); DOI:10.31579/2578-8868/112
Copyright: © 2020 Carlos Francisco Gutierrez Partida, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 19 December 2019 | Accepted: 22 January 2020 | Published: 27 January 2020
Keywords: spinal descompression; endoscopic; HD fluoroscopy
Endoscopic surgery has become an important tool in spinal surgery, the ergonomic design and the required length of the instruments, as well as the use of video monitors greatly affect our perception and performance. Some experts are resistant to the use of the endoscope in spinal surgery, because of the limitations in the perceptual information and that this can lead us to commit incorrect actions during the surgical procedure. Since the introduction in 1997 by Smith and Foley of a system consisting of progressive tubular dilators (MED) to later place an endoscopic vision system, the technique has become increasingly popular to this day. Based on this, other authors have documented the use of this endoscopic tubular system called Easy-Go reporting good results, so the authors of this article focus on the intraoperative peculiarities, experience, first impressions and the technical note of this system. (EASY-GO)
Endoscopic surgery has become an important tool in spinal surgery, the ergonomic design an the required length of the instruments, as well as the use of video monitors greatly affect our precpetion and performance. Some experts are resistant to the use of the endoscope in spinal surgery, because of the limitations in the perceptual information and that this can lead us to commit incorrect actions during the surgical procedure [5].
Nonetheless, the new improvements and introductions to new endoscope equipment Full HD, and some 3D have shown important results with images commensurable with microscope [1,15]. Since 2007 the high definition HD cameras with LED light are available to endoscopid neurosurgical procedures [6].
Furthermore, since the introduction in 1997 by Smith and Foley of a progressive tubular dilators system (MED) that later it had an endoscopic vision system, the technique has become increasingly popular to this day [2]. Actually this system (MED) it is not only for disectomy, also for a great variety of pathologies, like lumbar stenosis descompression [10,3,16] among others.
The idea of minimally invasive suergery decrease the tissue damage [7,8,9,11,12,13,14] and postoperatories discomfort, demands the quest and development of new techniques and instrumental like ilumination system and magnification [4].
Based on this, other authors [6] have been documented the use of the tubular endoscopic system called Easy-Go, reporting good results and proposing a learning curve(6,19) and less extensive training. If exists a nonconformity respect of the use of this new endoscopic system, we have the resource to make the inmediate exchange for the microscopic. While we acquaint with this new technology, consequently the authors of this article focus on the intraoperative peculiarities, experience, first impressions and the technical note of this system. (Easy Go).
Material and Methods:
Endoscopic system:
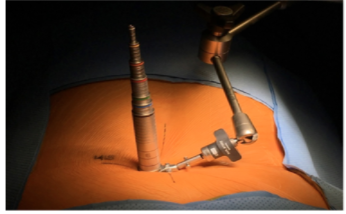
The “Easy Go [Gaab-Oertel]” system, consists in a progresive tubular dilators to do a Transmuscular surgical acces (Figure.1).
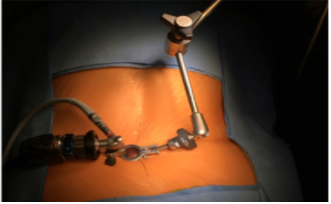
The surgical procedure is done through a tube with a exterior diameter of 19 mm (Figure.2).
croscopic sight, they have to work in a complete endoscopic sight through a second generation 25º Hopkins-ll optic, the optic can be rotate 270º through the holder of this. Also they have different endoscopic lenghts as well as tubes and diameters to allow flexible positions and different depths. The optic is set to the work deck and then to the surgical table.
Surgical procedure:
The surgical procedure has to be under general anesthesia, in some cases used total intravenous anesthesia (TIVA).
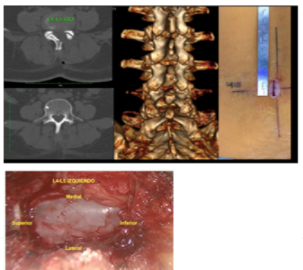
The patient will be in prone-decubitus position, previuous asepsia and antisepsia of the area. Placement of the surgical field, under sight in real time with fluroscopy, make a surgical mark of the area.
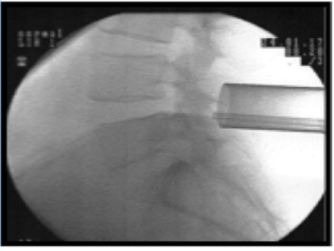
A para-medial incision is made with length of 2 cm, the skin is opened and incise the posterior thoracolumbar fascia and spinal erector muscle fascia, a tube holds to the article arm, previously fixed to the surgical table and then the adapter of the tube gets the position for the optic sight of 25º Hopkins-ll (Figure.3). Starts the bimanual endoscopic time (Figure.4).
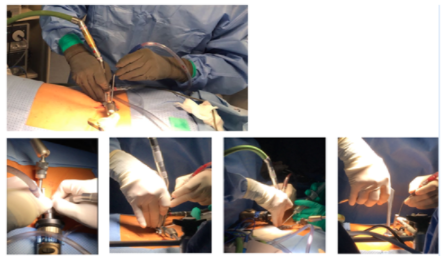
Starts the miller of the lamina with drill bit match head 14MH30 of high speed (MidasRexMR) and Kerrison punch forceps, the flavum ligamentum is visualized and retired, the entrance area of the intertransverse foramen is explored taking in consideration the lateral ipsilateral recess and then tilt the tube and have a oblique sight of the entrance of the same area and make the same procedure comented for the bilateral descompression trough an unilateral surgical access, descompression is corroborated to “ complacency” of the surgeon, hemostasia is corroborated and close the surgical incisión by planes. Drains are not placed in any case (Figure.5).
Results:
After any procedure, you have to make an analysis about the problems, advantages and disadvantages tan the Easy Go-ll system presents.
In the first cases, it was always necessary to contain the microscope ready, when we were in the transition and acquaint with the tubular endoscopic equipment, with the objective to change for a 3D vision with the microscope in the pertinent moment. . Ocasionally we realized the change to the microscope because the decompression was considered too slow and was necessary that followed the chronology of the surgical time in the room of operations and in other occasions by fault of precepction of depth or the no suitable identification of the anatomical structures doing that the surgeon does not seat unsuspecting and/or comfortable regarding the decompression. In two cases we did not have the microscope forcing us therefore to realize the decompression in his whole with the endoscopic system and this generarted more confidence for the following cases, in which it did not have microscope.
The progresive tubular dilator system developed by Smith and Foley [2] was created to treat lumbar hernias, today this system is aplicated for another pathologies of the spine, for example; spinal descompresión by lumbar, cervical or thoracic stenosis among others. The time show us satisfactory results of this technique because is a minimally invasive procedure [17,18]. We adopt this new system since 2017 because in some cases we are not available to have a microscopic and this endoscopic tubular system is portable, flexible an dynamic. Within of the advantages of this system is that the surgical procedure if the surgeon can not feel confortable he can exchange the 2D vision for the 3D vision inmediatly whitout need to lost the surgical deck, this way the surgeon will be training to perform surgeries progressively with the endoscopic system. We can corroborate than the learning curve and the training is fast and short [9], minimizing the surgical times.
In the last years there have been discovered minimal invasive endoscopic techniques with advantages and desadvantages, this system is one of the neurosurgical arsenal (20). Netherless the present study does not excludes any option about the literature. Finally we considered that more studies required in the future for the long term follow up whit this technique to show the advantages and desadvantages of this system.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
